Before we get to Ozempic, semaglutide, and the billion-dollar GLP-1 drug industry, we need to talk about a study from 2004 that the wellness internet mostly got wrong. Nilsson and colleagues published a paper in the American Journal of Clinical Nutrition that has been misread ever since. Twelve healthy volunteers. Test meals matched on carbohydrate content. Whey protein versus white bread as a reference. The result: whey produced 90% higher insulin AUC than bread, despite producing 57% lower blood glucose AUC.
Same subjects. Same study. Same day. Whey raised insulin dramatically more than bread did — while raising blood sugar dramatically less. This one data point has been used to argue that whey protein causes insulin resistance, that protein spikes are dangerous, and that people concerned about metabolic health should avoid whey. Every one of those conclusions is wrong. Understanding why requires understanding what insulin actually does — and what GLP-1 has to do with it.
The Distinction That Changes Everything
There are two different questions about insulin that get conflated constantly in nutrition discourse. The first is: does this food acutely raise insulin? The second is: does habitual consumption of this food cause insulin resistance? These are not the same question, they do not have the same answer, and confusing them produces exactly the kind of half-true health advice that has people avoiding egg whites and chicken breast on the grounds that protein spikes insulin.
Acute postprandial insulin is physiological. Your pancreas evolved to release insulin after meals. Every meal that contains protein, carbohydrate, or a combination of both will produce an insulin response. This is not pathology. This is normal endocrine function. The pancreatic beta cell detects rising amino acid concentrations, rising glucose, and incretin hormones from the gut wall, and it releases insulin in response to that signal. Insulin then does its job: it facilitates amino acid uptake into muscle for protein synthesis, it facilitates glucose clearance from blood, and it signals adipose tissue and liver about the fed state. Insulin appearing after a meal is not a problem. It is a solution.
Chronic fasting hyperinsulinaemia is pathological. When fasting insulin is chronically elevated — not because you just ate, but because peripheral tissues have become resistant to insulin's signal and the pancreas is compensating by producing more — that is the metabolic disease state. Fasting insulin above 10 mIU/L, HOMA-IR above 1.5, triglycerides rising, HDL falling, GGT trending upward within the normal range: this is the decade before prediabetes that standard testing misses. This has nothing to do with whey protein.
The “insulin from whey is dangerous” argument maps a half-true rule — carbohydrates raise insulin — onto a different question: what drives metabolic disease? Acute postprandial insulin from a protein-rich food that simultaneously lowers blood glucose is not the metabolic problem most people think it is. It is the opposite of the metabolic problem.
The GLP-1 Mechanism — What Ozempic Is Mimicking
GLP-1 — glucagon-like peptide 1 — is an incretin hormone produced by L-cells in the small intestine and colon in response to food arrival. It has four primary actions: it stimulates insulin secretion from pancreatic beta cells (amplifying the glucose-clearing response), it suppresses glucagon (preventing the liver from releasing glucose into already-elevated blood), it slows gastric emptying (delaying how fast food leaves the stomach and reduces the speed of glucose entry into the bloodstream), and it acts on the hypothalamus to signal satiety — reducing appetite and food-seeking behaviour.
Semaglutide (Ozempic, Wegovy) and liraglutide (Victoza, Saxenda) are GLP-1 receptor agonists — synthetic molecules that bind to and activate the GLP-1 receptor more potently and for longer than natural GLP-1, which has a half-life of approximately two minutes in circulation. The drugs work by doing what GLP-1 does naturally, but more powerfully and for longer. The clinical effects — better glucose control, reduced appetite, slower gastric emptying, weight loss — are the pharmacological amplification of a physiological mechanism that food has been triggering since the first vertebrate intestine encountered a meal.
Protein is the most potent natural stimulus of GLP-1 release among the three macronutrients. Specifically, the amino acids leucine, isoleucine, valine (branched-chain amino acids), lysine, and threonine — abundantly present in whey — stimulate L-cell GLP-1 release directly. This is the mechanism behind the whey insulin response. Whey raises insulin not because it is metabolically disruptive, but because it powerfully stimulates the normal gut hormone cascade that makes insulin secretion appropriate, glucose clearance effective, and appetite signals meaningful. The 80% higher GIP (gastric inhibitory polypeptide, another incretin) response to whey seen in the 2007 Nilsson follow-up is part of the same story.
Pre-Meal Protein — The Clinical Application
The mechanistic understanding produces a directly practical protocol: consuming protein 15–30 minutes before a carbohydrate-containing meal produces meaningfully better postprandial glucose control than consuming the same food together or without the protein pre-load.
The mechanisms are compounding. GLP-1 is released by the protein, slowing gastric emptying before the carbohydrate arrives. Insulin is primed by the incretin response before glucose enters the bloodstream, producing faster and more effective glucose clearance. CCK (cholecystokinin) is released by protein arrival in the small intestine, amplifying satiety signalling and further slowing gastric transit. The carbohydrate that follows enters a gut that is already signalling satiety, a blood sugar regulatory system that is already primed, and a gastric emptying mechanism that is already slowed.
In type 2 diabetes and prediabetes, this protocol has been studied directly. A randomised crossover trial by Jakubowicz et al. showed that 25–30g of whey consumed 30 minutes before breakfast significantly reduced postprandial glucose excursions compared to consuming the same breakfast without the pre-load. This is not alternative medicine. This is the same mechanism that GLP-1 receptor agonist drugs exploit pharmacologically, applied through food.
The Satiety Index — What This Connects To
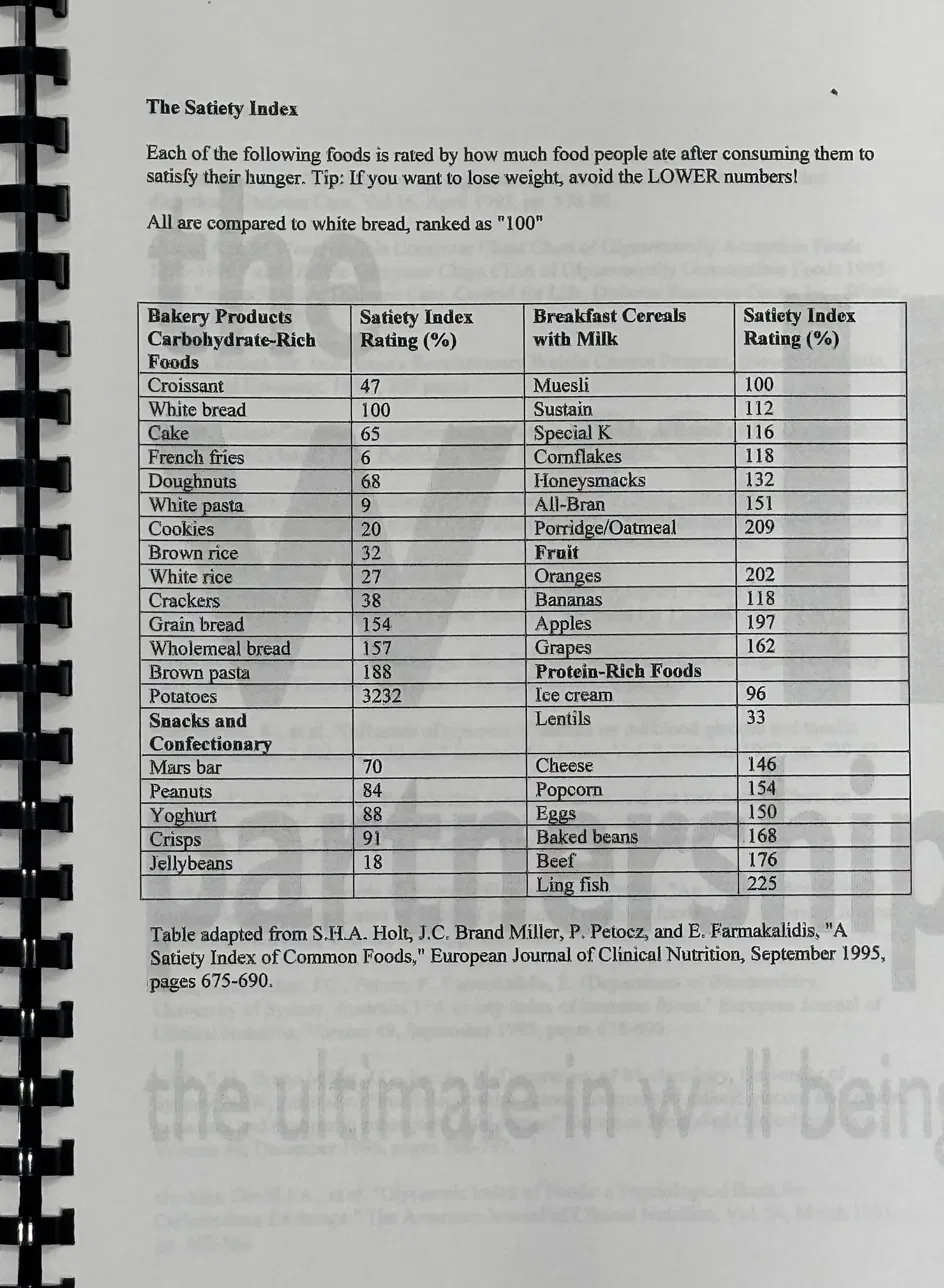
Susanna Holt’s 1995 Satiety Index, published in the European Journal of Clinical Nutrition, measured the satiety produced per calorie across 38 common foods, with white bread as the 100% reference. Boiled potatoes scored 323% — three times the satiety of bread per calorie. Croissants scored 47%. Fish, oat porridge, and oranges scored consistently high. The finding that challenged the prevailing carbohydrate-as-satiety narrative: many high-protein and high-water-content foods produced substantially more satiety than their glycaemic index or calorie content would predict.
The mechanism Holt identified — that protein, fibre, volume, and water content independently predicted satiety per calorie — is the same mechanism that drives GLP-1 drug efficacy. Protein stimulates GLP-1 and CCK directly. Fibre slows gastric emptying and feeds the gut bacteria that produce secondary GLP-1-stimulating signals. Volume and water content activate gastric mechanoreceptors that contribute to satiety signalling. Foods that are simultaneously high in protein, fibre, volume, and water content — eggs, fish, legumes, root vegetables — naturally activate multiple satiety pathways simultaneously. Foods that are calorie-dense, low in fibre, and low in protein — processed snacks, refined starches, liquid calories — bypass most of them.
The GLP-1 drug craze is not new science discovering new biology. It is pharmacology amplifying biology that has been understood, at the food level, for thirty years. The practical implications were always available without a prescription. They required understanding what food does at the mechanistic level and building meals accordingly — which is a harder sell than a weekly injection, but produces the same fundamental physiological result through a less invasive, less expensive, and reversible mechanism.
What This Means in Practice
Lead every meal with protein
25–30g of protein at the start of every meal — before the carbohydrate arrives — primes GLP-1, CCK, and insulin. This is not about protein being inherently superior. It is about the sequence of signals the gut sends to the regulatory systems.
Pre-meal protein for blood sugar management
If post-meal glucose excursions are a concern — HOMA-IR elevated, HbA1c trending upward, afternoon crashes — 20–30g of protein 20–30 minutes before the main carbohydrate load produces measurable improvement in the glucose response. Whey, eggs, or fish work equally well.
Choose high-satiety index foods
Boiled potatoes, fish, eggs, legumes, and oat-based foods consistently score highest on satiety per calorie. Ultra-processed foods consistently score lowest. The practical implication: a diet built around high-satiety-index foods naturally reduces total calorie intake without calorie counting, because the satiety signals are proportionally stronger.
Liquid calories are the exception
Liquid calories — including fruit juice, smoothies, and caloric drinks — bypass the gastric mechanoreceptors and the full satiety cascade. They are absorbed rapidly, produce a sharp glucose response, and generate less satiety per calorie than their solid equivalents. This is why drinking 200ml of apple juice produces less satiety than eating two apples, despite identical calorie and sugar content.
The fear of protein raising insulin is based on a genuine observation applied to the wrong conclusion. Whey does raise insulin substantially. It also lowers blood glucose substantially, stimulates GLP-1 powerfully, triggers satiety signalling through multiple pathways, drives muscle protein synthesis, and — in the clinical literature on type 2 diabetes — reduces postprandial glucose excursions when consumed before a carbohydrate meal. These are the opposite of the metabolic harms the insulin-fear narrative predicts.
The drugs that have captured global attention for weight loss and blood sugar management work by amplifying a mechanism that food has always activated. Understanding the mechanism — rather than the drug that exploits it — gives you the practical tools to produce the same result through the foods that trigger it naturally. This is not a revolutionary insight. It is thirty years of satiety science, finally getting the attention it always deserved.