Nutrition · Weight Loss · Metabolism · Clinical Practice
Calories Matter —
But Not in the Way You've Been Told
The evidence that calories are at the top of the pecking order for weight management is real and worth taking seriously. Bryan Walsh's work on this is compelling. But calorie needs vary by up to 1,500 kcal per day before you account for individual variation. Damaged metabolism, disordered eating history, liver congestion, blood sugar dysregulation, and nutrient depletion all change how calories are processed. This is the clinical nuance that most calorie conversations never reach.
Stephen Duncan
BSc (Hons) · PG Dip · MSc · FDN-P · 37 Years Clinical Experience
June 2026
10 min read
Let me say the unfashionable thing first: calories matter. In the functional medicine and integrative nutrition space there is sometimes a tendency to dismiss calorie balance as an oversimplification — to focus so heavily on food quality, gut health, hormone balance, and metabolic individuality that the fundamental thermodynamic reality gets lost. Bryan Walsh, whose evidence-based approach to weight loss I respect considerably, makes this case clearly and with rigour: energy balance is the primary variable. You cannot consistently ignore it.
I have seen this personally. Trying to fight at under 67 kilos when my walk-around weight was 71 to 75 kilos means you learn, with some urgency, what caloric restriction actually does to a body — the fatigue, the mood shift, the performance degradation, and then the profound appreciation for real food that follows. That experience did not make me dismissive of calories. It made me respect them more.
What I am arguing here is not that calories don't matter. I am arguing that treating calorie balance as the only variable — or as a variable that operates identically in every person regardless of their metabolic history, hormonal environment, liver function, gut health, and nutrient status — is an incomplete clinical model that produces poor outcomes for a significant subset of people. Specifically, the subset who most need help.
The X-Factor problem — why calorie counting is harder than it looks
The diagram below is adapted from Paul Chek's work in How to Eat, Move and Be Healthy, drawing on John Berardi's research on energy expenditure partitioning. It illustrates something that most calorie-counting approaches ignore entirely: the enormous variability in what any given person actually needs on any given day.
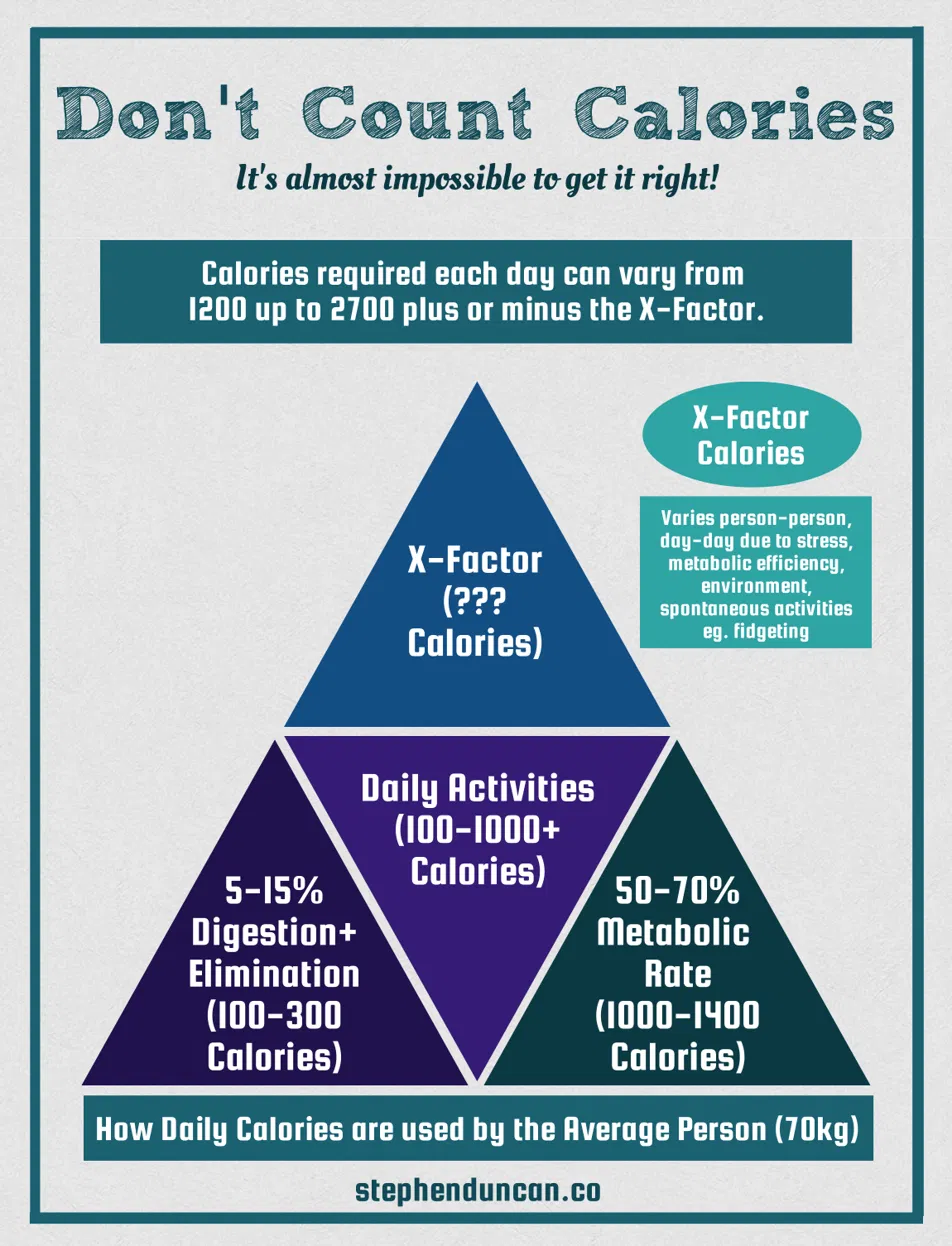
Daily calorie partitioning — adapted from Paul Chek / John Berardi. The X-Factor at the apex is the variable no app can calculate.
The base of the pyramid is resting metabolic rate — the calories required simply to keep the body alive. For an average 70kg adult this sits between 1,000 and 1,400 kcal per day, representing 50–70% of total daily energy expenditure. This is regulated by thyroid hormone, by mitochondrial density and efficiency, by lean muscle mass, and by the activity of the Na⁺/K⁺-ATPase pump described in the electrolytes post. It is not fixed. It varies with thyroid status, temperature, sleep quality, chronic stress, and dieting history — all of which suppress it.
Daily activity — exercise plus non-exercise activity thermogenesis (NEAT, which includes everything from walking to fidgeting to postural adjustments) — accounts for 100–1000+ kcal per day. The range is enormous because NEAT varies by up to 2,000 kcal per day between individuals at the same body weight doing the same formal exercise. This is not something you can accurately track with a fitness device. The error margin on wearable calorie estimates is 25–40% even in controlled conditions.
Digestion and elimination — the thermic effect of food — accounts for approximately 5–15% of daily expenditure: 100–300 kcal. Protein has the highest thermic effect (25–30% of protein calories are used in processing it), which is one of the clinical arguments for higher protein intake in weight management independent of satiety effects.
And then there is the X-Factor — the variable at the apex of the pyramid that no calorie calculator accounts for. Day-to-day variation in stress, metabolic efficiency, environmental temperature, spontaneous activity, illness, sleep deprivation, and individual genetic variation in metabolic rate. This can swing daily calorie needs by several hundred kilocalories in either direction. The overall range for an average person: 1,200 to 2,700+ calories per day before the X-Factor is added. That is a range of 1,500 kcal before you have even started to think about individual variation.
What raises the X-Factor
Cold exposure (thermogenesis). High training volume. Stress-induced sympathetic activation (cortisol drives gluconeogenesis — making glucose from muscle protein). Fever or immune activation. High NEAT — some people fidget constantly and burn 300+ kcal daily more than sedentary counterparts at the same body weight.
What suppresses the X-Factor
Chronic caloric restriction (metabolic adaptation — the body reduces NEAT and basal rate). Subclinical hypothyroidism. HPA axis depletion (cortisol supports resting metabolic rate — depleted HPA lowers it). Sleep deprivation. Nutrient depletion — particularly CoQ10, B vitamins, magnesium, and iron, all of which are required for mitochondrial ATP production.
"Calories are the top of the pecking order — and so is the question of why the calorie equation isn't working for this person, in this body, at this point in their life."
Where calorie counting works — and where it breaks down
For a metabolically healthy person with no significant dieting history, no hormonal disruption, adequate nutrient status, good liver function, and a stable relationship with food — calorie awareness combined with protein targets and food quality guidance produces good results. This is the population most nutrition research is conducted in. The approach works, and it works because the metabolic machinery is intact and the X-Factor is relatively stable.
The clinical population I see most frequently is different. Test results showing what I would call a damaged metabolism — suppressed resting metabolic rate, impaired thyroid conversion (T4 to T3), elevated cortisol driving muscle catabolism, insulin resistance impairing fat oxidation, and nutrient depletions affecting every step of the energy production pathway. For this person, reducing calories further into an already-deficient system is not the primary intervention. It can make things actively worse.
You also hear the language of intent without the reality of execution. "I'm eating well and training hard" — but with pasta and alcohol in the mix at the weekend. "I'm off it" meaning the occasional drink, not none. These are not moral failures. They are the honest complexities of human behaviour around food that a calorie calculator cannot accommodate. And with significant liver congestion and blood sugar instability, the Friday indulgence can be enough to undo five days of careful effort — not because the person lacks willpower, but because their metabolic processing of those foods is impaired at a biochemical level.
The upstream blockers — what has to be addressed before calories become the primary lever
01
Thyroid function
Subclinical hypothyroidism (TSH above 2.5, low-normal Free T3) suppresses basal metabolic rate and impairs fat oxidation. Calorie restriction in this context accelerates the metabolic adaptation — the body conserves energy more aggressively. TSH, Free T3, Free T4, and reverse T3 must be part of any clinical weight management picture.
02
HPA axis and cortisol pattern
Chronic elevated cortisol drives visceral fat deposition and muscle catabolism simultaneously. The person gaining fat despite caloric restriction and exercise is often in HPA Stage 1 or 2 — activated cortisol driving gluconeogenesis and fat storage around the midsection. The DUTCH cortisol pattern tells you whether caloric restriction will produce results or simply add to the physiological stress load.
03
Insulin resistance and blood sugar
Hyperinsulinaemia locks fat in adipose tissue by inhibiting hormone-sensitive lipase — the enzyme that releases stored fat for oxidation. You cannot out-calorie-deficit a significant insulin resistance. Fasting insulin, HbA1c, and fasting glucose on blood chemistry identify this. HbA1c of 5.74% (in the upper normal range) is already beginning to indicate impaired glucose regulation that warrants dietary management before calorie counting.
04
Liver congestion
The liver is the primary metabolic organ — responsible for fat oxidation, glycogen storage, gluconeogenesis, and the conversion of T4 to active T3. A congested liver impairs all of these. Elevated GGT on blood chemistry is often the first visible sign. Alcohol, even in modest weekend quantities, produces a significant hepatic burden that depresses fat oxidation for 48–72 hours after consumption.
05
Nutrient depletion
Mitochondrial fat oxidation requires B vitamins (particularly B2, B3, B5), CoQ10, magnesium, iron, and L-carnitine as cofactors. Restricting calories without addressing nutrient depletion reduces the substrate available for the metabolic processes that calorie restriction is supposed to activate. This is the clinical reason why adequate protein and nutrient-dense food matters more than calorie density for the depleted population.
A more useful framework — quality, timing, and quantity in that order
The framework I have used clinically for many years — and that preceded many of the current evidence-based weight management approaches — puts quality first, timing second, and quantity third. This is not anti-calorie. It is a sequencing argument: the quality of what you eat determines the nutrient density and hormonal response; the timing determines insulin rhythm and metabolic flexibility; and the quantity — calories — is the final calibration once the first two are in place.
The Practical Framework
Quality → Timing → Quantity — in that order
- Protein target first. 1.6–2.2g per kg of body weight daily depending on starting point, activity level, and lean mass goals. Protein is the macro with the highest thermic effect, the strongest satiety signal, and the most critical role in preserving muscle during a caloric deficit. Get this right before worrying about anything else.
- Eat protein, fat, and fibre before carbohydrate at each meal. Meal sequencing reduces the glycaemic impact of carbohydrates consumed later in the meal — not by eliminating them but by blunting the insulin spike. This is practical, evidence-based, and requires no calorie counting.
- Stabilise blood sugar before restricting calories. Erratic blood sugar creates cortisol spikes, drives cravings, and impairs fat oxidation. Three meals with adequate protein and fat, no snacking, consistent timing — before calorie reduction is introduced.
- Address the upstream blockers. Thyroid, cortisol pattern, liver function, nutrient status. A calorie deficit applied to a dysfunctional metabolic system frequently produces fatigue, muscle loss, and hormonal disruption without meaningful fat loss.
- Then apply calorie awareness. Once the above are in place, modest caloric restriction (250–500 kcal deficit) combined with adequate protein produces consistent, sustainable fat loss without the metabolic adaptation that aggressive restriction triggers.
Making weight — what I learned the hard way
I mentioned earlier the experience of fighting at under 67 kilos with a walk-around weight of 71–75 kilos. What I learned from that period was not the theoretical limits of caloric restriction but its lived consequences: the flatness in training, the irritability, the poor sleep, the mental preoccupation with food that eating disorders research recognises as a physiological response to energy restriction rather than a psychological failing.
The key insight that took too long to arrive was the distinction between being lean and being depleted. You can be at a low body weight and profoundly nutrient-deficient — low iron affecting oxygen transport to muscles, low B vitamins impairing energy production, low magnesium disrupting sleep and recovery. The scales say one thing. The test results say another. The performance tells you a third story entirely.
That experience is why I now start weight management clients not with a calorie target but with a blood chemistry panel. The metabolic picture — thyroid, iron status, liver enzymes, fasting glucose, B12, vitamin D, and a basic hormonal assessment — tells me whether the body is capable of responding to a caloric deficit with fat loss or whether we are asking a depleted system to do more work it cannot currently support.
"The question is not whether calories matter. They do. The question is whether this person's metabolism is in a state where a calorie deficit will produce fat loss — or whether something upstream needs to be addressed first."
The weekend factor — and why honesty matters more than perfection
One of the most consistent patterns in clinical weight management is the gap between the weekday picture a client describes and the weekend picture they minimise. "I'm eating really well" — but pasta and alcohol on Friday and Saturday. "I'm off it" — meaning they've reduced, not eliminated. "I had a bad weekend" — meaning two significant alcohol episodes and the associated dietary loosening that follows.
None of this is a character flaw. It is the reality of how most people live, and a calorie-counting approach that treats every day identically fails to account for it. The clinical question is not whether the weekend indulgences are "allowed" — that is a diet psychology question. The clinical question is whether, in this person with their specific metabolic picture, the weekend pattern is enough to undo the weekday work. For someone with significant liver congestion, insulin resistance, and an already-suppressed metabolic rate — it very often is.
The most useful thing I can do in that situation is not lecture about the alcohol or the pasta. It is to show the test results that make the mechanism visible. When a client can see their GGT trend alongside their weekend habits, or understand that their fasting insulin tells a specific story about why fat loss has stalled despite genuine effort, the motivation to address it comes from understanding rather than restriction. That is always the more durable change.
What Testing Shows in Weight-Resistant Clients
The most consistent findings in clients who are eating carefully, exercising regularly, and not losing weight: TSH above 2.5 with low-normal Free T3 (subclinical hypothyroidism suppressing BMR), fasting insulin above 8 µIU/mL (hyperinsulinaemia locking fat stores), elevated GGT (liver congestion impairing fat oxidation and T4 conversion), low ferritin (iron insufficiency reducing mitochondrial efficiency), low vitamin D (impairs insulin sensitivity and thyroid receptor function), and depleted B vitamins and magnesium on organic acids testing (mitochondrial ATP production bottlenecks). These are not reasons to abandon calorie management. They are reasons to address the metabolic environment before expecting calorie management to work efficiently.
Understand your metabolic picture before your next diet
The TDG blood chemistry assessment covers thyroid function, fasting insulin and glucose, liver enzymes, iron status, vitamin D, B12, and inflammatory markers — the upstream variables that determine whether your metabolism is in a state where caloric restriction will produce the results you are working toward. Test first. Then work with the results.
Book a Strategy Call →