I started coaching athletics and boxing at eighteen. That hands-on reality — working with real people who responded differently to identical programmes, identical diets, identical recovery protocols — was my first lesson in the thing that would eventually define my entire clinical practice: individual variation is not noise in the data. It is the data. The same programme doesn’t work for everyone because people are not the same. This seemed obvious to me then. It still seems obvious to me now. It remains, despite everything, consistently ignored by mainstream dietary and health guidance.
What follows is not a complete account of thirty-seven years of continuing education. It is the highlights — the sources, people, publications, and moments that genuinely changed how I think. I’m writing it partly because I’m in the process of clearing out decades of accumulated printed material — books, newsletters, conference notes, photocopied papers — and there’s something worth preserving in the history of how clinical knowledge was actually acquired before Google Scholar, before podcasts, before the algorithm decided what you should know next.
The formal education was a BSc Honours in Developmental Biology at the University of Glasgow, followed by an MSc in Coaching Studies with Applied Sports Science. The developmental biology degree gave me something that still underpins everything: a cellular-level understanding of how biological systems actually work. Enzyme kinetics. Signal transduction. Gene expression. The kind of biochemistry that makes functional medicine findings interpretable rather than mysterious. Understanding why ferritin is relevant to thyroid conversion, or why beta-glucuronidase reactivates conjugated oestrogen — these are not things you pick up from a nutrition course. They require a grasp of molecular biology that sits beneath the clinical application.
The thesis title is worth noting: the effects of antiandrogens on testicular descent. Environmental antiandrogens — synthetic chemicals that block or mimic androgen signalling during development — are the same endocrine disruptors that appear in the heavy metals and mould posts, in the DUTCH hormone metabolite patterns, and in the clinical consequences of glyphosate and phthalate exposure. The research question I was asking in 1992 in the Department of Anatomy is the same question the DUTCH Plus oestrogen metabolite pathways are answering in clinical practice today. The tools changed. The obsession did not.
My kinesiology and biomechanics lecturers gave me the physics of human movement — kinematics, kinetics, forces, moments, the geometry of load on joint structures. My lecturer Simon Coleman in particular drilled into me the details: where hands, elbows, shoulders, head, scapulae, pelvis, hips, knees, and feet should be in position and angles during movement; the timing, sequence, and rhythms of muscular activation. I didn’t know at the time that this foundation would eventually connect to Paul Chek’s inner and outer unit core training, to Shirley Sahrmann’s movement impairment syndromes, and to the visceral manual therapy I would later study. The dots only connect in retrospect.
Before the internet was a research tool, before PubMed was publicly accessible, before podcasts, before Instagram, before the algorithm — there were magazines. And if you were in health, fitness, or strength training in the early 1990s, and you wanted the genuine applied science rather than the mainstream press release version, you subscribed to specific publications and read them cover to cover.
The covers tell a story that needs some context. This is what the distribution mechanism looked like — the vehicle that carried serious applied science to practitioners, trainers, and athletes who had no other way to access it. PubMed wasn’t publicly searchable until 1997. There was no functional medicine podcast, no evidence-based Instagram account, no algorithm curating research for you. If you wanted to know what was actually happening in human physiology, performance nutrition, and supplement science, you read publications like these. The image on the cover was how they competed for newsstand space. The content inside was why serious practitioners kept subscribing.
I knew these publications were not without bias. MM2K was essentially a vehicle for EAS supplements, and I knew that. Muscular Development had advertisers who shaped what could be said and what couldn’t. But buried in the sponsored content were genuine contributors who understood training science and biochemistry, who were working with elite athletes and advanced physique competitors, and who were drawing on the actual literature rather than repeating received wisdom. You had to filter. But the filtering itself was an education — learning to identify when something was marketing and when it was science was a clinical skill that has served me ever since.
The reading strategy I developed then has never changed. When I come across a recommendation, a claim, or a protocol, the first question is always: what is the proposed mechanism? If there is no mechanism — if it’s just correlation, authority, or tradition — that doesn’t automatically make it wrong, but it places it in a different epistemic category than something with a clear mechanistic explanation supported by multiple lines of evidence. Dan Duchaine was not right about everything. But he was asking the right question — what is actually happening at the cellular level — at a time when most fitness culture was not asking it at all.
The year was 1996. I was still learning to use email. Websites weren’t really a thing yet for ordering products. My research methodology consisted of reading those bodybuilding magazines and pulling out the threads that connected to actual physiology.
One day I came across an article in Muscle Media featuring Oscar de la Hoya — a favourite boxer at the time — kneeling on a Swiss ball, doing reaction training with tennis balls. Something clicked immediately. This wasn’t just balance training. This was nervous system training. Teaching the body to respond under instability, to fire the right muscles in the right sequence when the ground beneath you couldn’t be trusted. The article mentioned Paul Chek.
I ordered my first Swiss ball over the phone. That is literally how you did it in 1996. I got the number from a Paul Chek Seminars catalogue that arrived by post. The ball was white, anti-burst rated. I called him Mr White. Partly after Reservoir Dogs. I became obsessed with learning to move on an unstable surface — bench pressing, flyes, eventually standing on it, golf swings, boxing punches — and I watched Paul Chek’s videos obsessively. What Chek taught, and what I gradually absorbed over years, was not just core training methodology. It was an integrated view of human performance: the relationship between nutrition and movement, between stress and recovery capacity, between nervous system function and training adaptation. His concept of work-in and work-out — that the nervous system has a finite stress budget and intense exercise is a withdrawal, not just a deposit — changed how I prescribed training fundamentally.
Around 1998 or 1999 I discovered Uffe Ravnskov’s work — a Swedish physician who had done what I should have done years earlier: he questioned the data behind the cholesterol-heart disease hypothesis. He read the actual research. He found the holes, the inconsistencies, the selectively presented findings that told one story while quietly ignoring evidence that told another.
Reading Ravnskov was like watching a magic trick explained. Once you see how it’s done, you cannot believe you fell for it. I had a degree in science. I understood biochemistry and endocrinology. I could read research. And I had still believed the prevailing narrative for years because it came wrapped in institutional authority — respected bodies, major studies, government guidelines, media consensus. Questioning all of that felt presumptuous. That is how good institutional mistakes persist. Not because people are stupid, but because the epistemic cost of dissent feels too high.
After Ravnskov I pulled out my biochemistry textbooks and mapped cholesterol synthesis from the ground up. What actually happens at the molecular level. The synthesis pathways, the regulatory mechanisms, the roles cholesterol plays in every steroid hormone, in every cell membrane, in bile acid production. This exercise — going back to the molecular biology rather than the clinical guideline — has become my default response to any clinical claim I find suspicious. The mechanism is always the most reliable place to look.
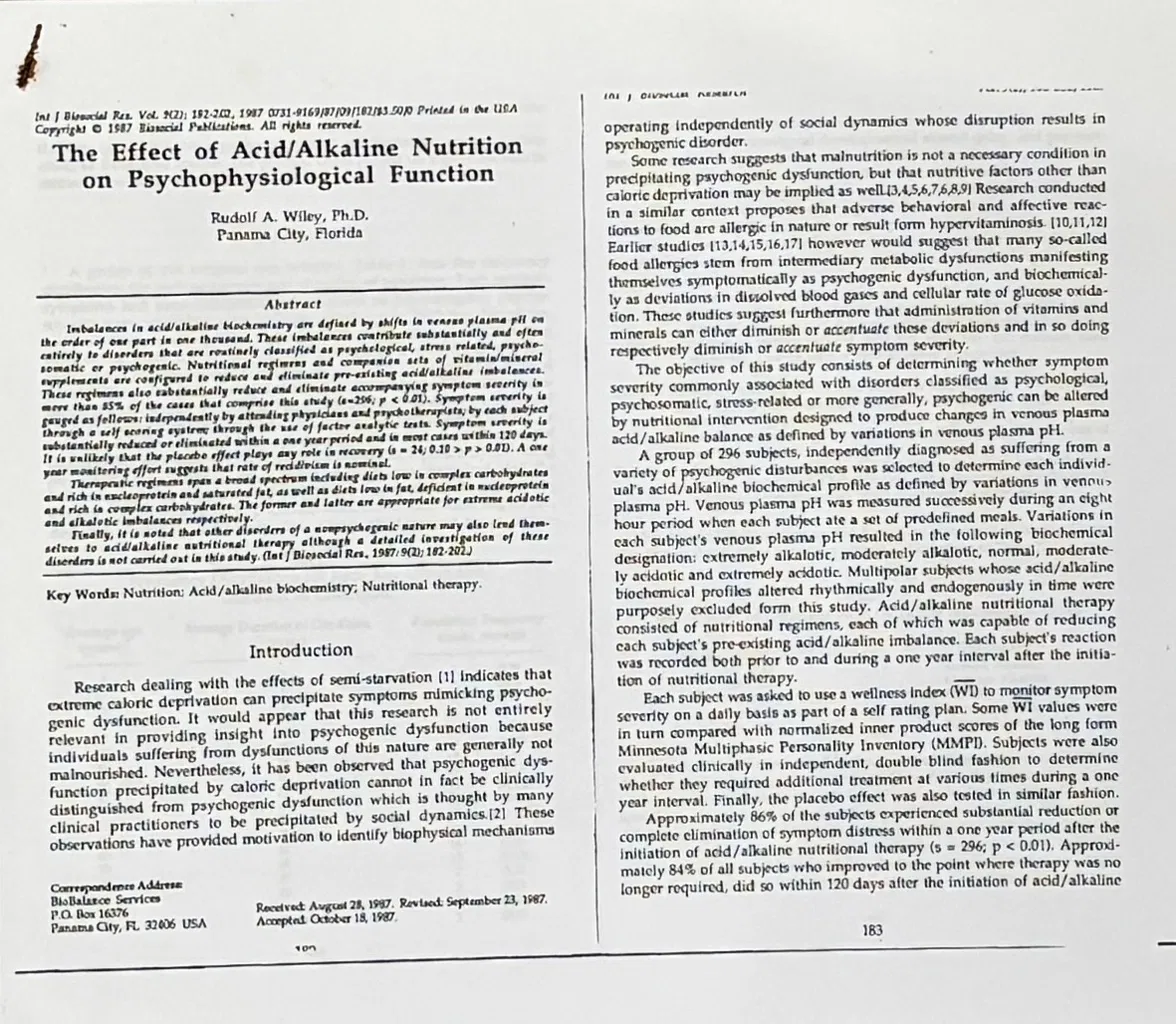
Around this time I came across a paper that I still have — printed out, physically in my possession — that challenged the then-dominant alkaline diet narrative in a way no mainstream publication was doing. It was: The Effect of Acid/Alkaline Nutrition on Psychophysiological Function by Rudolf A. Wiley PhD, published in International Journal of Biosocial Research, Vol. 9(2), 182–202, 1987.
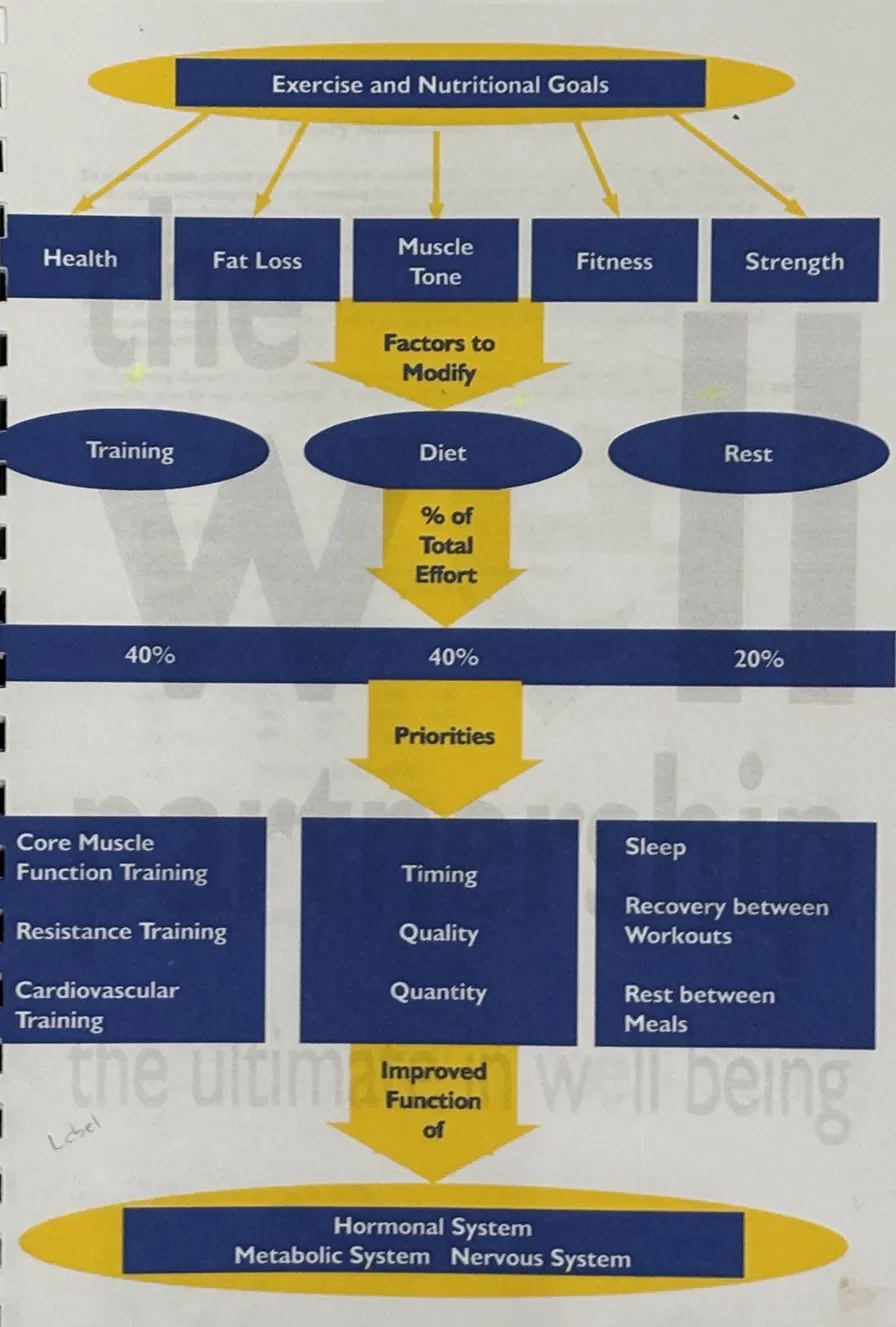
At the time, the alkaline diet was everywhere. Eat vegetables, make your body alkaline, achieve health. This became eat vegan to make your body alkaline, which became plant-based for the environment, which became dietary recommendations shaped as much by politics and climate policy as by individual physiology. I watched this evolution happen over two decades and found it consistently frustrating — not because vegetables are bad (they are not) but because the one-size-fits-all approach to anything drives me to distraction. The alkaline diet narrative treated individual metabolic variation as irrelevant. Wiley’s paper treated it as central. The paper connected acid/alkaline balance to autonomic nervous system type — which eventually led me to Bill Wolcott’s metabolic typing work, and to the clinical framework that now sits at the foundation of everything I do nutritionally.
Individual variation is not noise. It is the signal.

In September 2001 I attended the 1st International Conference on Movement Dysfunction in Edinburgh — a conference that brought together some of the most important thinkers in musculoskeletal physiotherapy and rehabilitation. The line-up included physiotherapist Mark Comerford on movement control testing, and a name I had already encountered through Paul Chek: Shirley Sahrmann.
Sahrmann’s work on movement impairment syndromes — the idea that pain is frequently caused by sustained movement habits that progressively load specific structures beyond their tolerance — connected directly to what I had been trying to understand clinically for years: why some clients had pain that no structural diagnosis explained, why the same diagnosis produced completely different functional limitations in different people, and why correcting technique and movement patterns frequently resolved pain that orthopaedic medicine had declared structural and therefore permanent. Hearing her speak and reading her book cover to cover was one of those relatively rare experiences where theoretical understanding and clinical observation simultaneously resolve.
Also at that conference was Paul Hodgkinson, who demonstrated ultrasound imaging of transverse abdominis and pelvic floor activation live with a volunteer from the audience. The foundational Hodges and Richardson paper — published in 1997 in Spine — had established that the transverse abdominis activates before limb movement regardless of direction, and before any other trunk muscle. This was not a reaction to expected force. It was an anticipatory feedforward activation — the nervous system preparing for movement before it occurs. This finding upended the rehabilitation model of reactive core training and established the transverse abdominis as a postural stability system, not a movement system.
What fascinated me then — and still does — is how this connects to everything downstream. A diaphragm that cannot drop fully on inhalation because of stress-induced thoracic breathing, or because of visceral congestion in the upper abdomen, or because of poor thoracic mobility, cannot co-activate with the transverse abdominis properly. Intra-abdominal pressure regulation — the mechanism by which the spine is stabilised during movement — requires the diaphragm and pelvic floor to work in concert with the TA. When breathing is poor, core stability is poor, regardless of how many dead bugs or planks a person performs. And when core stability is poor, pain patterns emerge that look structural but are fundamentally neuromuscular and behavioural.
Around this same period I completed a weekend course with a French osteopath in visceral manipulation — Barral’s methodology — specifically to better understand the ileocaecal valve, which kept appearing in the case histories of people with alternating constipation and diarrhoea labelled as IBS. I had studied the parietal and visceral peritoneal layers in developmental biology and through Thomas Myers’ Anatomy Trains. The visceral manipulation course gave me the palpatory framework for what I was reading in the anatomy — and the clinical insight that the ileocaecal valve is not just a passive anatomical junction but a functional valve whose dysfunction has downstream consequences for colonic motility, abdominal pain patterns, and bowel habit that most gastroenterologists never assess.
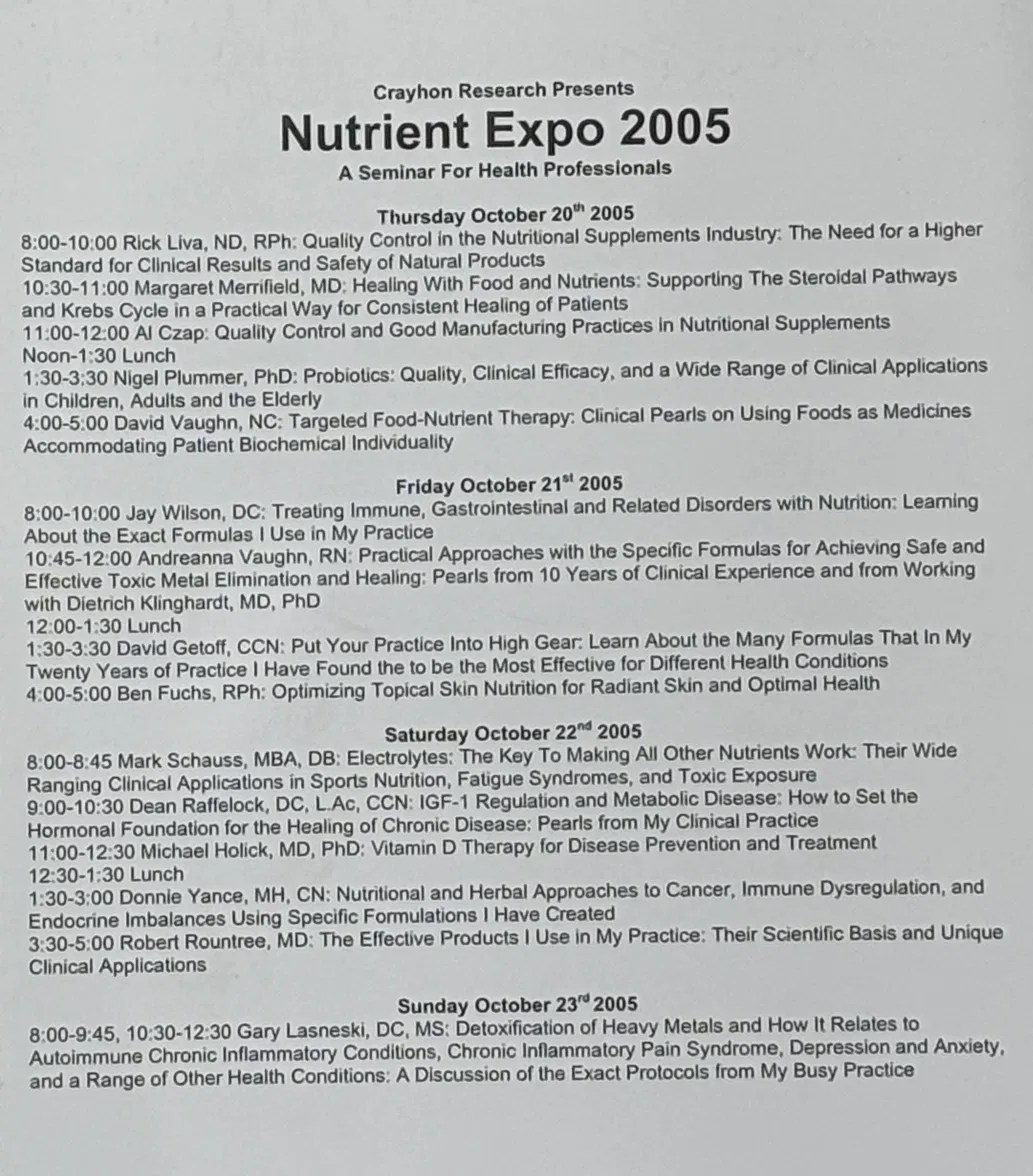
One of the most practically useful education experiences I have had was attending the Nutriex speaker presentations — clinicians, researchers, and formulation scientists speaking directly about the realities of supplement production. Not marketing materials. Not sales presentations. The actual science and economics behind what ends up in a capsule that can be sold at retail.
The names at those events included Mark Schauss, David Getoff, Andreanna Vaughn, Dietrich Klinghardt, Nigel Plummer, Michael Holick, and Rick Liva — people who were at the interface of research, clinical application, and commercial production. What I learned there has shaped every supplement recommendation I have made since.
The dose that produces an effect in a clinical study is frequently not the dose you can put in a capsule that retails at a price people will actually pay. The form of a nutrient used in research is frequently not the form used in a mass-market supplement — because the research form costs ten times as much. GMP (Good Manufacturing Practice) certification means the product contains what it says on the label — it says nothing about whether what is on the label is the right thing at the right dose. And excipients — the fillers, binders, flow agents, and coating materials that make a capsule manufacturable — can interfere with absorption, cause reactions in sensitive individuals, and in some cases antagonise the active ingredient they are supposed to deliver.
None of this means supplementation is ineffective. It means that the gap between what the research shows works and what is commercially available is larger than most people realise — and that navigating that gap requires understanding what to look for, not just reading a product label.
The formal functional medicine training came through Reed Davis and Functional Diagnostic Nutrition — the framework that brought the testing methodology I had been developing informally into a systematic clinical structure. The FDN-P programme covered blood chemistry at functional reference ranges, stool analysis, hormone testing, organic acids, and — most importantly — the clinical reasoning framework for integrating findings across tests rather than reading each one in isolation. Bill Wolcott’s Healthexcel Metabolic Typing training added the nutritional individualisation layer that the Wiley paper had first pointed me toward twenty years earlier.
I am going through these printed newsletters, conference programmes, and photocopied papers as I clear the shelves, and what strikes me is the quality of the thinking in some of them — the Peak Performance newsletters in particular. Dense, mechanistic, referenced, written by people who had spent years in the physiology literature and were translating it for practitioners and serious athletes. There is nothing equivalent today. There is more information available than at any point in history, and the average quality of publicly circulated health information is simultaneously the lowest it has ever been.
The algorithm optimises for engagement, not accuracy. The most shareable health content is the simplest content — the five tips, the one weird trick, the dramatic before and after. Clinical depth does not go viral. Nuance does not get shared. The result is that the internet has produced a paradox: more access to information has produced less informed consumers of that information, because the distribution mechanism actively selects against the kind of careful, mechanistic, individually contextualised thinking that actually changes health outcomes.
I am not nostalgic for dial-up internet. I use PubMed daily. I find papers in seconds that would have taken weeks to locate in 1995. But I am grateful that my clinical education was built on sources that required effort to obtain and time to digest — because that process of searching, ordering, waiting, reading slowly, and applying carefully produced a kind of clinical judgment that instant information access does not naturally build. The internet tells you facts. Long experience of applying them to people who respond unexpectedly tells you what the facts mean.
If any of this resonates — if you recognise the gap between what you’ve been told and what your biology is actually telling you — that is exactly the gap the Detective Health approach exists to close.