I wrote my first client diet guide at 28. It was called “A Greater Understanding Provides for Greater Control — The Gospel According to The Well Partnership.” It ran to approximately fifty pages. It covered meal timing, hormonal body composition, the roles of insulin, testosterone, cortisol, and growth hormone, protein thermogenesis, the satiety index, glycaemic load, the anabolic versus catabolic stress distinction, and the importance of sleep and recovery as active components of a body composition programme rather than afterthoughts. It had original diagrams. It had references. And it was given free to every client who wanted to understand what they were doing and why.
I did not think of it as unusual at the time. This was what the science said. This was what serious practitioners were teaching. The information was available — in academic journals, in the better sports science publications, in the specialist conferences that existed before the internet made everyone simultaneously an expert in everything and deeply confused by the contradiction. The challenge was not finding the information. It was synthesising it into something a client could act on.
What follows is a brief record of what the science said then — and what it still says now, repackaged for a market that has been systematically discouraged from remembering that it already knew.
Meal Timing — The Science That Predates Intermittent Fasting Influencers by Decades
The fundamental principle of nutrient timing — that the same calorie consumed at different times of day is partitioned differently between liver, muscle, and fat — was not invented by the intermittent fasting movement. It was established in the metabolic research literature of the 1970s and 1980s and was being applied in practical nutrition programming by the mid-1990s. The principle is mechanistic: insulin sensitivity varies across the circadian cycle, peaking in the morning and declining through the afternoon and evening. Carbohydrates consumed in the morning are more likely to be directed toward glycogen storage in muscle and liver. The same carbohydrates consumed late in the evening are more likely to be directed toward triglyceride synthesis in the liver.
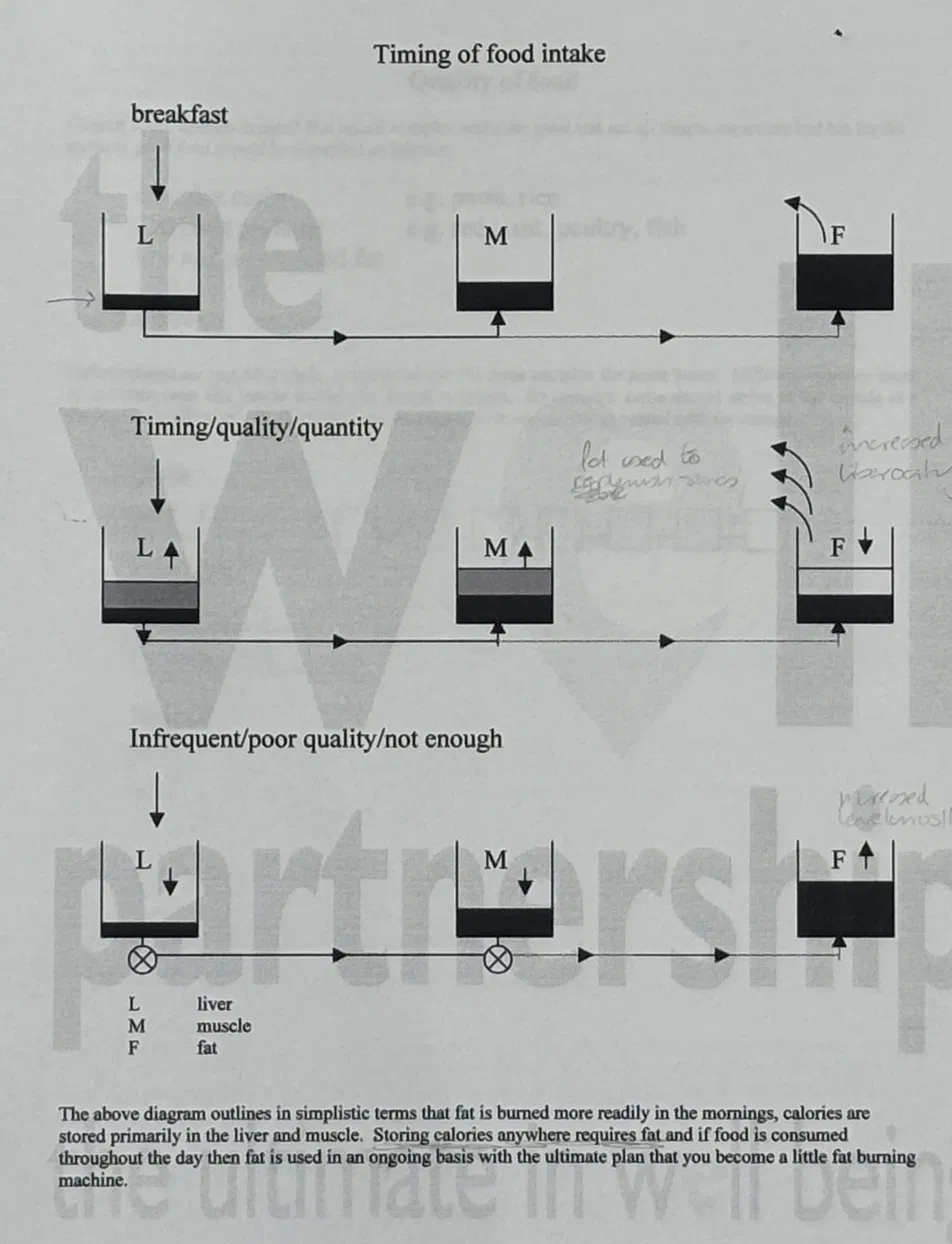
The diagram above — drawn for clients in the mid-1990s — illustrates three meal timing scenarios: correct timing with breakfast (liver and muscle stores filled, fat not expanding), optimal timing/quality/quantity (liver and muscle levels rising, fat declining), and infrequent/poor quality (liver and muscle depleted, fat accumulating). The arrows are direction of flow. The blocked pipes show shutdown of the partitioning mechanism. This is basic metabolic physiology applied practically. It predates intermittent fasting as a branded dietary approach by a decade and a half.
Insulin Partitioning — Before HOMA-IR Was a Household Term
The role of insulin as a partitioning hormone — directing calories toward either muscle and liver glycogen or adipose tissue triglycerides depending on the metabolic environment at the time of consumption — was understood in the sports science and endocrinology literature by the early 1990s. The clinical application was straightforward: create an insulin-sensitive environment through resistance training, adequate protein, and meal frequency, and the same insulin response to food directs more calories toward lean tissue and fewer toward fat stores. Create an insulin-resistant environment through chronic stress, poor diet, sedentary behaviour, and inadequate recovery, and the same insulin response does the opposite.
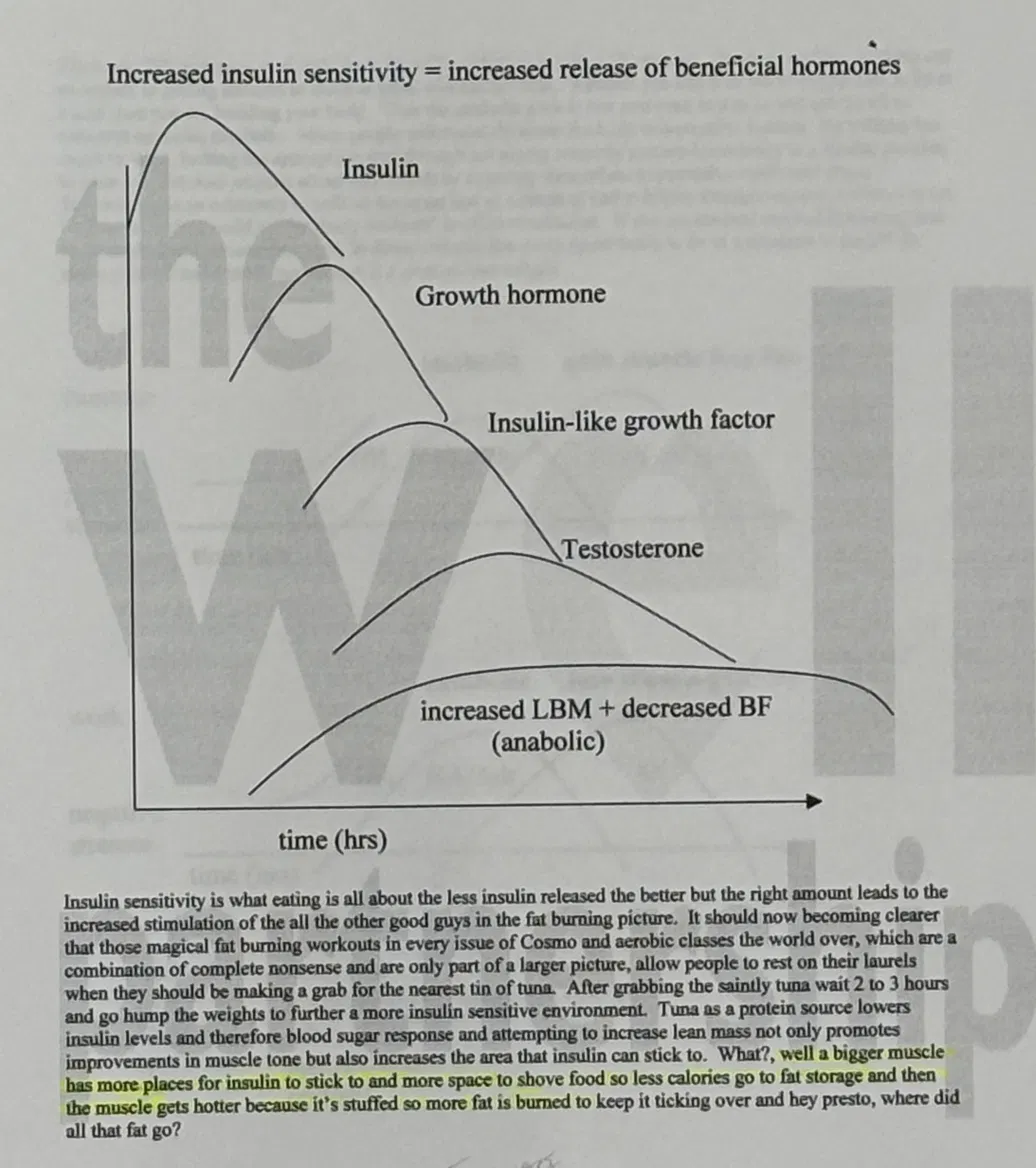
The cascade shown above — increased insulin sensitivity leading sequentially to growth hormone release, IGF-1, testosterone, and ultimately increased lean body mass with decreased body fat — is mechanistically accurate and was understood at the time. The clinical tool for measuring whether this cascade is functioning — fasting insulin and HOMA-IR — is now available to any practitioner. In the 1990s the assessment was indirect: body composition, performance, recovery, and symptom pattern. The test-don’t-guess approach has made explicit what was previously inferred.
The Testosterone-Cortisol Ratio — Before It Appeared on Magazine Covers
The testosterone-to-cortisol ratio as a marker of recovery and adaptation was not invented by the bodybuilding magazines of the 1990s, though they helped disseminate it. It emerged from the sports science literature in the 1980s as a practical index of whether an athlete’s training was producing anabolic adaptation or catabolic breakdown. High testosterone relative to cortisol indicated the body was in a building state. Elevated cortisol dominating testosterone indicated catabolic overreaching — training beyond the capacity to recover.
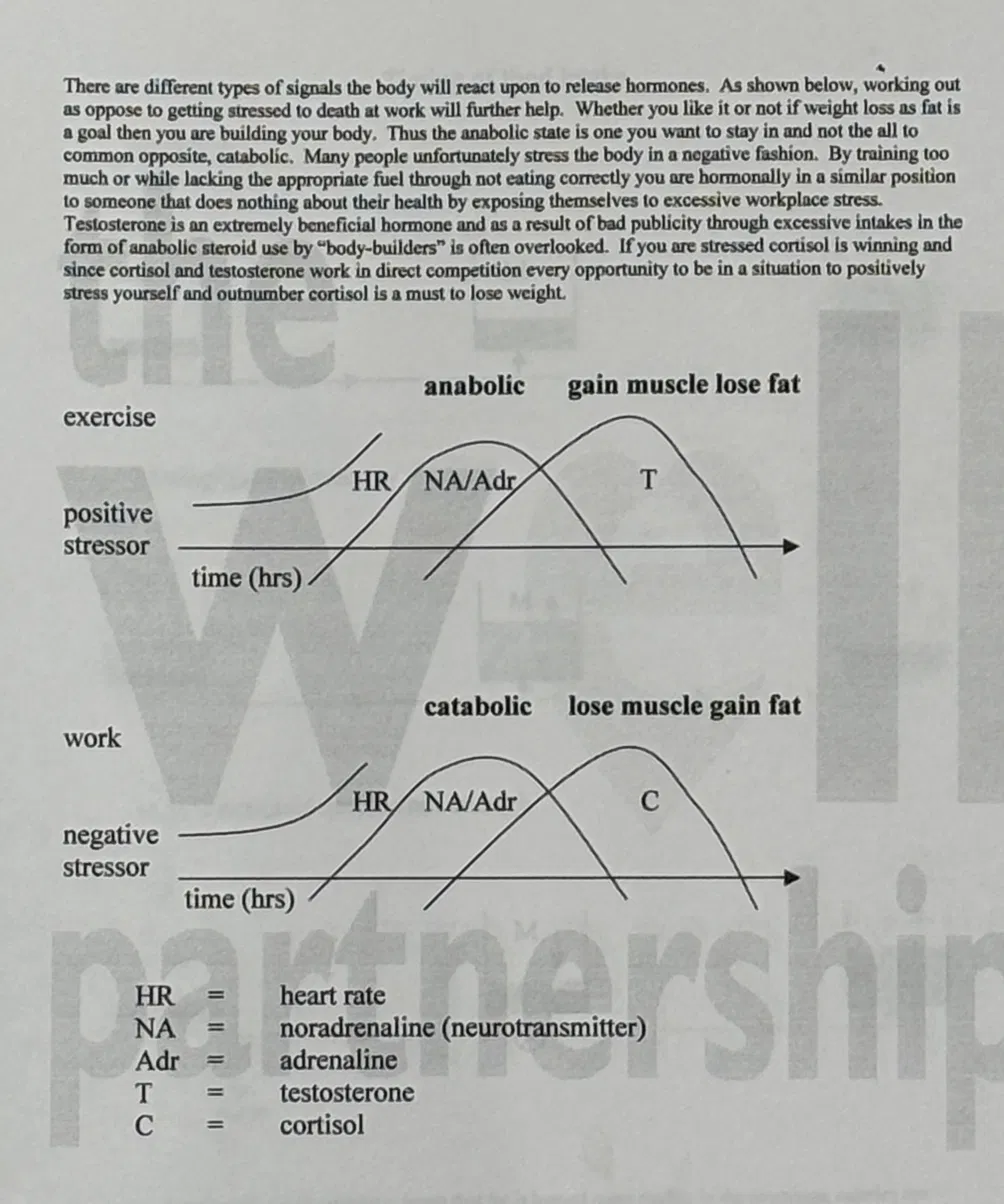
The practical implication — that a person who is chronically stressed at work and sleeping poorly will not achieve significant body composition improvement regardless of how hard they train, because the cortisol environment will dominate any testosterone adaptation signal — was being taught to clients in the mid-1990s. It is now confirmed by the DUTCH Plus diurnal cortisol pattern and the HOMA-IR correlation with visceral adiposity. The physiology was understood. The testing tools that make it measurable and specific to an individual are new. The mechanism is not.
Protein Thermogenesis — Before “Protein Is Satiating” Became Content
The thermogenic effect of protein — that approximately 18–25% of protein’s caloric value is consumed in the process of its own digestion, compared to 8% for carbohydrate and 2–3% for fat — was established in the metabolic literature by the mid-1980s and was being used in practical nutrition programming by the early 1990s. The implication is direct: a calorie of protein has a lower net caloric contribution than a calorie of fat or carbohydrate, because a larger proportion of its energy is dissipated as heat in the process of deamination, transamination, and gluconeogenesis. This is not new information. It has been on the nutrition literature for forty years.
The Obesity Epidemic Is Not a Knowledge Gap
The question that this history raises is uncomfortable: if the science was established thirty years ago and is essentially unchanged, why is the obesity rate in developed countries higher now than at any point in recorded history? Why are GLP-1 drugs prescribed to approximately 15% of adults in some Western populations? Why is metabolic syndrome — a cluster of conditions that the 1990s sports science literature already understood how to prevent — now the dominant health crisis of the twenty-first century?
The answer is not a knowledge gap. It is not that people do not know that protein is satiating, or that meal timing matters, or that sleep affects body composition, or that ultra-processed food bypasses satiety mechanisms. Most people know this. The problem is the gap between knowing and doing — the intention-behaviour gap that the psychology of change post addresses — and the structural environment that makes the low-satiety, high-reward, cheap, convenient food the path of least resistance for a tired, time-poor, chronically stressed population.
Thirty years of improved food science communication has not produced thirty years of improved dietary behaviour, because the distribution mechanism that carries the information — social media, algorithmic content, thirty-second videos — optimises for engagement rather than understanding. And the commercial interests that profit from processed food, pharmaceutical intervention, and diet culture cycling — fail, feel bad, buy the next solution — are considerably better funded than the practitioners who have been teaching the same mechanistically sound principles since the 1990s because they were true then and remain true now.
The science of body composition is not complicated. Adequate protein, appropriate meal timing, insulin-sensitive training, cortisol management through sleep and stress reduction, and food choices that activate satiety mechanisms rather than bypassing them. This was the framework in 1996. It is the framework in 2026. The GLP-1 drugs that are now generating billions in pharmaceutical revenue are doing pharmacologically what this framework produces nutritionally — at ten thousand times the price and with a side effect profile that boiled potatoes have never produced.
What Has Actually Changed
The tools have changed. In the 1990s, the assessment of insulin resistance was indirect — body composition measurement, performance tracking, symptom pattern. Now fasting insulin and HOMA-IR give a direct quantitative measure. The DUTCH Plus shows the complete hormonal picture in a way that was simply not available outside of research settings in 1996. The GI-MAP identifies the gut dysbiosis that impairs insulin signalling, drives inflammation, and disrupts the hormonal environment that body composition depends on. The Organic Acids Test shows whether the cells are producing energy efficiently or under oxidative stress. The Hair Tissue Mineral Analysis shows whether the minerals required for insulin signalling — chromium, magnesium, zinc — are depleted.
What this means is that the clinical framework for body composition is now testable rather than inferred. The mechanisms understood in the 1990s can now be confirmed, quantified, and personalised with functional testing. A person who is not losing weight despite doing “everything right” now has a systematic investigation available that can establish whether the problem is hormonal (DUTCH), gut-derived (GI-MAP), mitochondrial (OAT), or mineral-based (HTMA) — rather than defaulting to the conclusion that they are not trying hard enough.
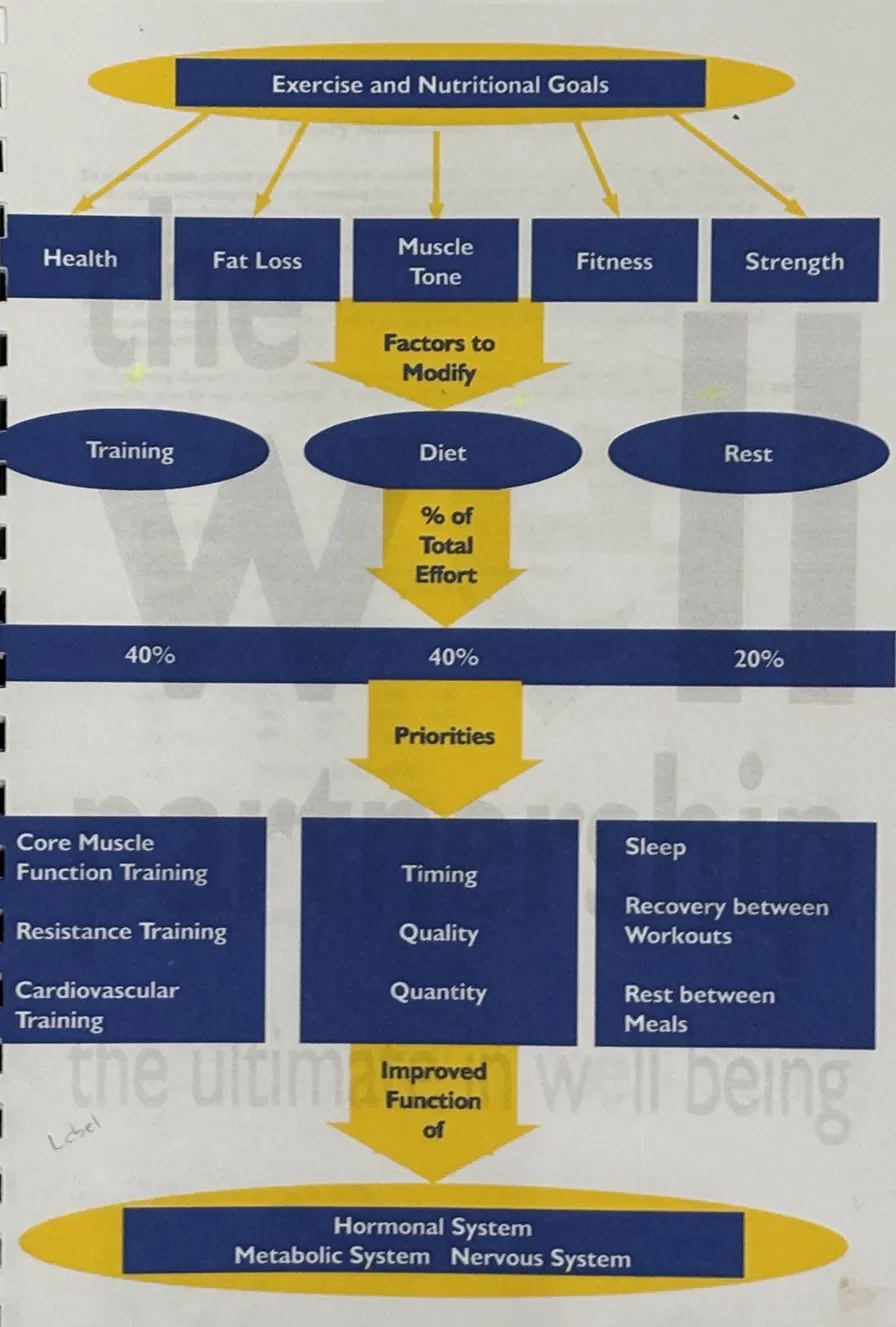
The framework in the diagram above — drawn in the mid-1990s for clients who wanted to understand the integrated picture — maps Training, Diet, and Rest each at their weighted contribution to the outcome, with the priorities within each pillar listed, and the three systems that the combined effect improves: hormonal, metabolic, and nervous system. That is the same architecture as the TDG five-test programme, which now assesses hormonal function through the DUTCH, metabolic function through blood chemistry, and nervous system and stress through the DUTCH CAR and HRV data. The understanding was there. The measurement tools have caught up.
The science of body composition has not changed substantially in thirty years. What changes is the packaging, the platform, the commercial vehicle, and the price. GLP-1 drugs work. So does a diet built around high-satiety foods, adequate protein, appropriate meal timing, regular resistance training, quality sleep, and managed cortisol. The drug option requires a prescription, costs hundreds of pounds per month, and produces weight regain in the majority of people who stop taking it because the underlying behaviour and biological environment have not changed. The food and lifestyle option produces durable change because it addresses the underlying system rather than pharmacologically overriding one component of it.
A greater understanding still provides for greater control. It did in 1996. It does now.